As edited by Christian75 (talk | contribs) at 15:47, 9 March 2020 (Undid revision 944722027 by 77.118.29.50 (talk) Removing the added t from:…phenoxy-(t’’S’‘)-phospho…). The present address (URL) is a permanent link to this version.

In a new publication in Nature Plants, assistant professor of Plant Science at the University of Maryland Yiping Qi has established a new CRISPR genome engineering system as viable in plants for the first time: CRISPR-Cas12b. CRISPR is often thought of as molecular scissors used for precision breeding to cut DNA so that a certain trait can be removed, replaced, or edited. Most people who know CRISPR are likely thinking of CRISPR-Cas9, the system that started it all. But Qi and his lab are constantly exploring new CRISPR tools that are more effective, efficient, and sophisticated for a variety of applications in crops that can help curb diseases, pests, and the effects of a changing climate. With CRISPR-Cas12b, Qi is presenting a system in plants that is versatile, customizable, and ultimately provides effective gene editing, activation, and repression all in one system.
“This is the first demonstration of this new CRISPR-Cas12b system for plant genome engineering, and we are excited to be able to fill in gaps and improve systems like this through new technology,” says Qi. “We wanted to develop a full package of tools for this system to show how useful it can be, so we focused not only on editing, but on developing gene repression and activation methods.”
It is this complete suite of methods that has ultimately been missing in other CRISPR systems in plants. The two major systems available before this paper in plants were CRISPR-Cas9 and CRISPR-Cas12a. CRISPR-Cas9 is popular for its simplicity and for recognizing very short DNA sequences to make its cuts in the genome, whereas CRISPR-Cas12a recognizes a different DNA targeting sequence and allows for larger staggered cuts in the DNA with additional complexity to customize the system. CRISPR-Cas12b is more similar to CRISPR-Cas12a as the names suggest, but there was never a strong ability to provide gene activation in plants with this system. CRISPR-Cas12b provides greater efficiency for gene activation and the potential for broader targeting sites for gene repression, making it useful in cases where genetic expression of a trait needs to be turned on/up (activation) or off/down (repression).
Scientific Reports volume 9, Article number: 3928 ( 2019 ) Cite this article.

HONG KONG — Pet cats and dogs cannot pass the new coronavirus on to humans, but they can test positive for low levels of the pathogen if they catch it from their owners.
That’s the conclusion of Hong Kong’s Agriculture, Fisheries and Conservation Department after a dog in quarantine tested weakly positive for the virus Feb. 27, Feb. 28 and March 2, using the canine’s nasal and oral cavity samples.
A unidentified spokesman for the department was quoted in a news release as saying. “There is currently no evidence that pet animals can be a source of infection of COVID-19 or that they become sick.”

3 minutes for glaucoma eye surgery.
Cataract and glaucoma are eye diseases that progress by aging. Both are severe diseases that can cause blindness, but in Japan, unique treatment methods and causes are being investigated. For cataracts, the world is paying attention to a Japanese doctor who has devised an innovative surgical method which is in just over 3 minutes. And distinctive research is progressing at Japanese universities as to what kind of ingredients can delay the progression of glaucoma. How can we save people from blindness? Explore with us the forefront of Japanese ophthalmic medical care.
:oooo.
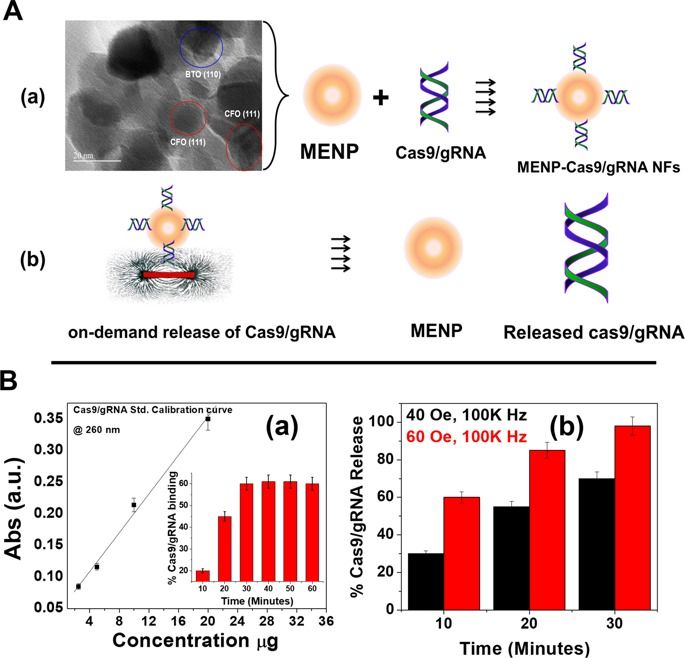
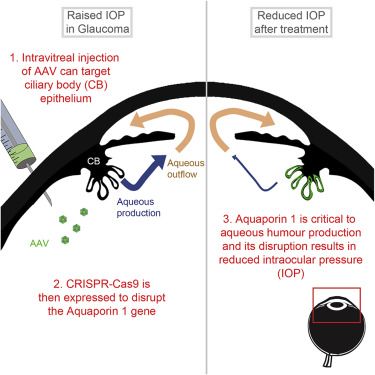
A novel approach to treat glaucoma is reported that achieves reduced intraocular pressure by combining intravitreal adeno-associated virus (AAV) gene delivery to the ciliary body with selective CRISPR-Cas9-mediated disruption of Aquaporin 1. Translational viability is assessed using both human ex vivo ciliary body cultures and two experimental mouse models.

Even since Alexander Fleming stumbled across penicillin—the first antibiotic drug—scientists knew our fight with evolution was on.
Most antibiotics work by blocking biological processes that allow bacteria to thrive and multiply. With prolonged, low-dosage use, however, antibiotics become a source of pressure that forces bacteria to evolve—and because these microorganisms are extremely adept at swapping and sharing bits of their DNA, when one member becomes resistant, so does most of its population.
Even more terrifying is this: because the same family of antibiotics generally act on the same biological pathways, when bacteria generate a mutation that resists one type of drug, it often renders that entire family of drugs useless.
The National Institutes of Health is testing the antiviral drug remdesivir, which is also being studied in patients in China. Running trials during epidemics is tricky, but scientists learned a lot about how to conduct them during recent Ebola outbreaks.