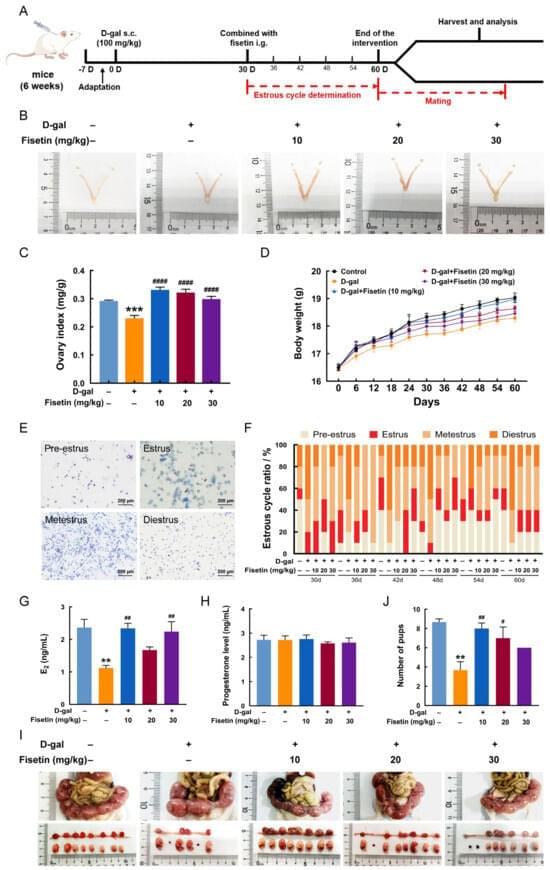
This study aimed to explore the alleviating effects of fisetin, a polyphenolic flavonoid, on ovarian dysfunction in a D-galactose (D-gal)-induced aging mouse model, as well as the underlying mechanisms, using both in vivo and in vitro experiments. Mice were subcutaneously injected with D-gal (100 mg/kg/day) for 60 days to establish the ovarian aging model; during the final 30 days, fisetin (10, 20, 30 mg/kg/day) was given orally. In addition, a senescent model of granulosa cell (GC) was established using D-gal and treated with fisetin. Fisetin supplementation improved ovarian endocrine function and reproductive capacity in aging mice, as reflected by regularized estrous cycles, elevated estradiol levels, and increased embryo numbers. Furthermore, fisetin reduced the number of atretic follicles and the extent of ovarian fibrosis and senescence, while simultaneously restoring the proliferation-apoptosis balance in follicular GCs, as well as alleviating oxidative stress. RNA-sequencing revealed that AMP-activated protein kinase (AMPK)/mechanistic target of rapamycin (mTOR) signaling and mitophagy were involved in the protective effects of fisetin against ovarian aging. Consistently, fisetin treatment promoted mitophagy, accompanied by AMPK/mTOR activation in ovarian tissues and GCs following D-gal exposure. Inhibition of AMPK attenuated the effect of fisetin on mitophagy. Additionally, blockage of mitophagy also reversed the beneficial effects of fisetin on mitochondrial injury, oxidative stress, cell cycle arrest, and cellular senescence in D-gal-induced senescent GCs. These findings indicate that fisetin prevents ovarian aging by suppressing follicular GC oxidative damage and ameliorating cell cycle arrest via activation of AMPK/mTOR-mediated mitophagy, thereby preserving female fertility.



{kind=link}